醫學|VO₂ max — 如何為妳我的生命儲值自由


不知道你有沒有想過這個問題
—— 在人生的最後十年想過怎麼樣的生活?
大家都會為了年老的自己存退休金,但能不能為未來的自己多做一些健康的儲值?除了留意定期健檢報告上的血壓、血糖、血脂之外,近期《美國醫學會雜誌》(JAMA)與《美國心臟病學院雜誌》(JACC)的大型研究都給出了一個結論:有一個健康指標,對死亡率與壽命的預測能力,甚至超越了高血壓、糖尿病或抽菸等傳統風險因子 。
這個指標相信有在做運動訓練的朋友都耳熟能詳
—— VO2 max(最大攝氧量)
在今年 1 月,挪威的三鐵運動員Kristian Blummenfelt 測得了有史以來最高的 VO2 max:101.1 ml/kg/min!同時越來越多的運動健身的網紅或教練,開始不由分說地吹捧 VO2 max,這樣合理嗎?關於VO2 max 的測量方法、男女數值上落差的原因、 Peter Attia 醫師提出的健康存摺觀念、想提升 VO2 max又該如何訓練?
有興趣就一起看下去吧!
本文Outline
什麼是VO2 max
性別與年齡的自然折舊
Peter Attia 的健康存摺觀念
如何測量VO2 max
如何提升VO2 max
總結——Moving and living freely in our marginal decade
更多運動醫學相關文章
什麼是最大攝氧量
為什麼稱之為健康的「終極感測器」?
1. 宏觀的身體排氣量
VO2 max(Maximal Oxygen Consumption)指的是人體在劇烈運動期間,肌肉與組織能夠利用氧氣的最高速率,單位為每分鐘每公斤體重所消耗的氧氣毫升數(mL/kg/min) 。
如果把身體比喻成一台汽車,可以類比為引擎的排氣量 :
- 大排氣量引擎:VO2 max 高的人,就像大排氣量的休旅車,不論是高強度運動、加速都有較充足的生理餘裕 。
- 小排氣量引擎:VO2 max 偏低的人,只要爬個樓梯或小跑步,引擎就會開始顫抖、熄火 。
2. 身體不同系統間的協作
VO2 max 同時也是體內多個系統協同運作的展現 :
- 呼吸系統 交換氣體的能力 。
- 心血管系統 供血的能力 。
- 循環系統 血液中血紅素與氧氣結合、運輸的速度 。
- 周邊肌肉細胞的「發電廠」——粒線體(Mitochondria)利用氧氣轉化為能量貨幣(ATP)的效率 。
當 VO2 max 偏低時,往往意味著上述某個或多個系統正在衰退,因此它是整體健康狀態的終極感測器 。
性別與年齡的自然折舊
1. 先天的性別差異
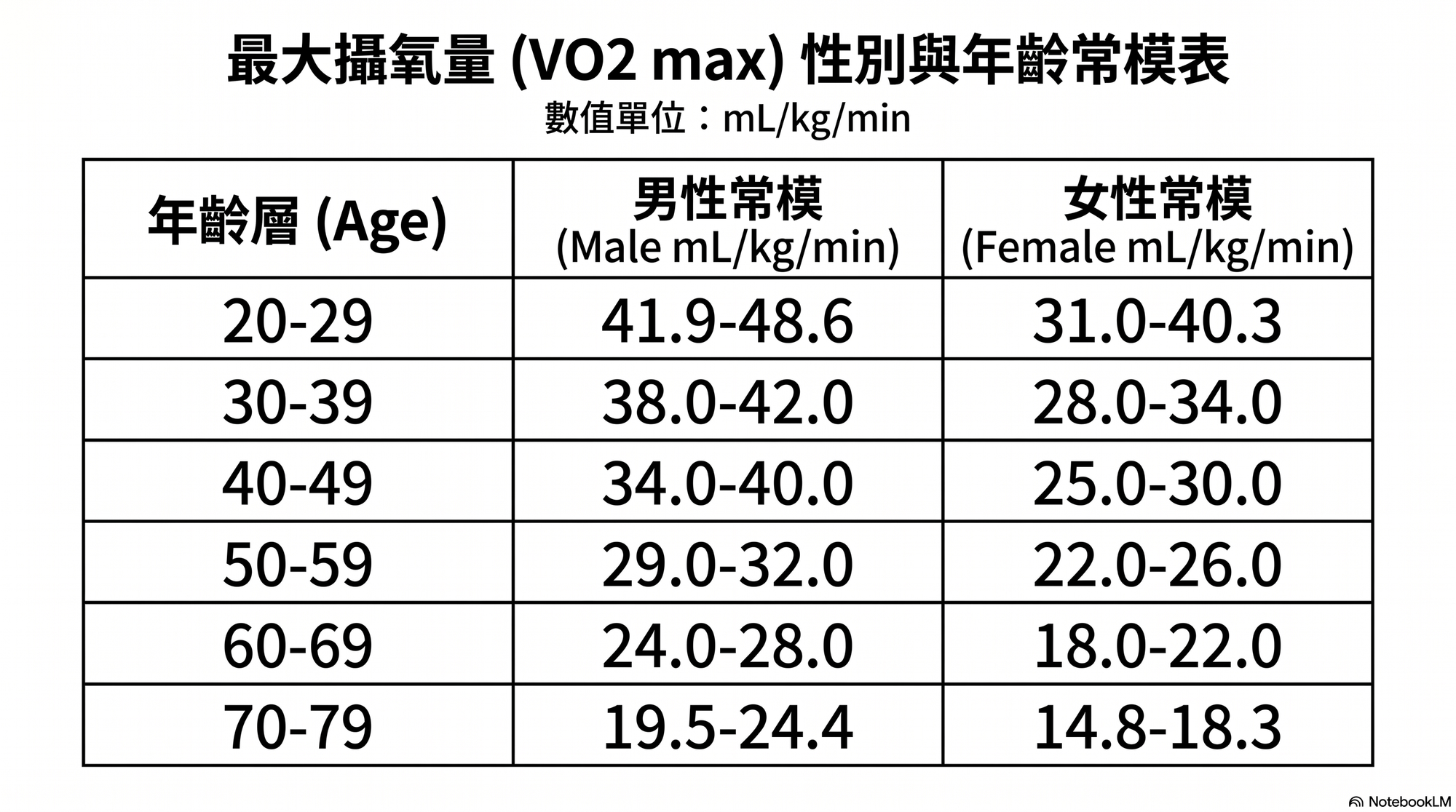
研究顯示男性的 VO2 max 平均高於女性約 10%-14% ,年輕男性平均約為 48.6mL/kg/min,女性約為 40.3 mL/kg/min 。 並非訓練量不足,這份差距主要源於心血管因素:女性的心臟體積、總血容量通常較小,且血紅素濃度比男性低約 10%,攜氧能力有所限制 。此外,女性在身體組成的脂肪比例較高,在運動中需要承載更多不產生能量的組織 。
2. 年齡的自然折舊
無論男女都面臨生物老化的殘酷。基本上VO2 max 在 30 歲後每十年下降 10%,過 50 歲後更會加速到每十年流失 15% 。
醫學上定義,一旦 VO2 max 低於 20 mL/kg/min,人體就會跨入「日常失能紅線」 ,此時心肺系統已無法負荷基本的日常行動。
健康存摺的觀念
我很認同現健康存摺觀念。就如同《長壽》(Outlive: The Science and Art of Longevity》的作者、同時也是一位醫師科學家的 Peter Attia 提出的論點:The Marginal Decade ——你生命中的最後十年想怎麼度過?是想要坐在輪椅上、過著生活無法自理的空活,還是能自己提行李出國旅行?這完全取決於你中年時存下了多少「健康資產」。
如果希望自己到了 100 歲依然能行動自如(VO2 max≥30),扣除掉自然老化折舊後的體能,在 40 歲時至少要具備 36 mL/kg/min 以上的實力(約等於 5公里能在 30 分鐘內跑完)。健康存摺、體能儲蓄的概念,即是年輕時體能上限存得越高,晚年衰退的坡道就相對越長,這樣一來才能延後失能。
如何測量最大攝氧量
測量與評估 VO2 max 主要有以下幾種方式。不同方式在精準度、成本與便利性上有所不同,形成了一套從「醫學黃金標準」到「日常智慧監測」的評估網絡。
實驗室氣體分析(換氣測量法):黃金標準
運動科學界與醫學臨床上公認最精準的測量方式,在醫學中心稱之為CPET (Cardiopulmonary Exercise Testing) 的心肺測試。
- 測量方式:受試者需要佩戴專用的呼吸面罩,並在跑步機或飛輪上進行「漸進式力竭運動測試」(Incremental Exercise Test) 。
- 科學原理:面罩連接的儀器會量測受試者在運動過程中,每一次呼吸所交換的氧氣(O2)與二氧化碳(CO2)的絕對體積 。當運動強度持續增加,而攝氧量達到飽和、不再上升時的最高速率,即為 VO2 max 。
- 除提供VO2 max的資訊以外,在醫學上,CPET也提供其他重要的資訊,包括協助診斷肺臟或心臟相關的疾病、開立運動處方及評估心肺復健後的進步等...,以前復健科住院醫師訓練我們要學習如何解讀這些測試後的複雜數據,若有興趣可先參考 Dr.M這篇運動測試的應用。
- 缺點與門檻:
- 費用高昂,在國外每次測量的費用大約需要200 美元 。台灣若非達到健保給付條件,也是一測就要好幾千塊。
- 測試極為痛苦: 受試者必須被逼到生理極限(力竭狀態) 。
- 非絕對無誤: 即便是實驗室測量也會因為操作方法或器材校正而有誤差。
智慧穿戴裝置:日常趨勢監測
這是目前大眾最普遍的追蹤方式。
- 測量方式: 配戴 Apple Watch 或 Garmin 等智慧手錶,在戶外進行跑步等有氧運動 。
- 原理: 智慧手錶主要是透過「心率」與「移動速度」的比例,並結合使用者的年齡、體重等背景資料,代入公式進行推估 。
- 精準度限制(平均約 13% 誤差): 2025 年發表在《PLOS ONE》上的臨床研究證實,智慧手錶的估算值平均誤差大約在 13% 左右,準確度較為參差不齊 。
- 手錶數據的「優化現象」: 有時候跑完一次高品質的間歇訓練(如挪威 4x4),隔天手錶數據會立刻「提升一格」 。這通常不是你一天之內變強了,而是因為你在高心率下成功維持住了高有氧配速,讓手錶的演算法優化了評估 。
Treat it as a measure, not a target!
- 實用價值:對於業餘運動員來說, VO2 max 可以是一個很有用的體能衡量標準 ,但應該著重於「改變的趨勢」,不要過度執著於精確的數字!
運動表現推估法
若沒有智慧手錶或預算做實驗室檢測,可以經典的耐力模型或跑步成績來推估。
在醫學上,若 VO2 max 低於 20 mL/kg/min 即屬於「日常失能紅線」(連基本的從椅子上站起來、打掃都會感到困難)。如果你在 30 分鐘內可以慢跑完 5公里,在中年時期大約代表你的 VO2 max 具備 36 mL/kg/min 以上的實力,若在 50 歲時能以 22 分鐘跑完 5 公里,則 VO2 max 大約落在 50 左右 。
如何提升最大攝氧量
大數據與運動科學的兩階段心肺定存策略
前言:打破「唯有高強度才能強心臟」的傳統迷思
在過去,許多教練與運動員普遍存在一個刻板印象,認為只有操到吐的高強度間歇訓練(HIIT)才能有效提升心血管功能與 VO2 max,而低強度的有氧訓練(如 Zone 2)只對周邊骨骼肌的適應有幫助。
然而,運動科學界的耐力訓練教科書——由知名運動生理學家與頂尖教練 Iñigo Mujika 主編的《Endurance Training, Science and Practice》明確指出
心血管表現與 VO2 max 的提升,本質上是「訓練強度」與「整體訓練量」兩者交互作用、區間重疊的結果(Overlapping Effects)。
前面提到的Peter Attia醫師也反對盲目的硬練,提倡「分區精準刺激」的健康儲蓄方針。另外近期 Garmin 分析數百萬名用戶的大規模數據也應證了:最大攝氧量與每週的「整體訓練量」呈現的線性成長。
- 單車數據: 每週騎乘 0–20 英里的騎士,平均 VO2 max 為 49;而每週騎乘 200 英里以上的發燒友,數值則飆升至 64,且在統計區間內「完全看不到瓶頸期」。
- 跑步數據: 每週跑超過 31 英里的跑者,其平均靜止心率從不運動者的 62 bpm 降到了優異的 55 bpm,展現了強大的總訓練量所帶來的心血管適應。
為了精準且高效地儲存體能,
現代運動科學提倡「雙軌複利、兩階段訓練法」
第一階段:大量 Zone 2 打底
- 訓練強度: 最大心率的 70%–80%。
- 體感判斷為「對話測試」(一邊運動一邊說話會稍微吃力)或 全程可舒適地用鼻子呼吸。
- 科學原理: 根據教科書的「區間重疊圖」,心血管系統的輸送能力(Pump)影響範圍其實跨越了 Zone 1 到 Zone 6。
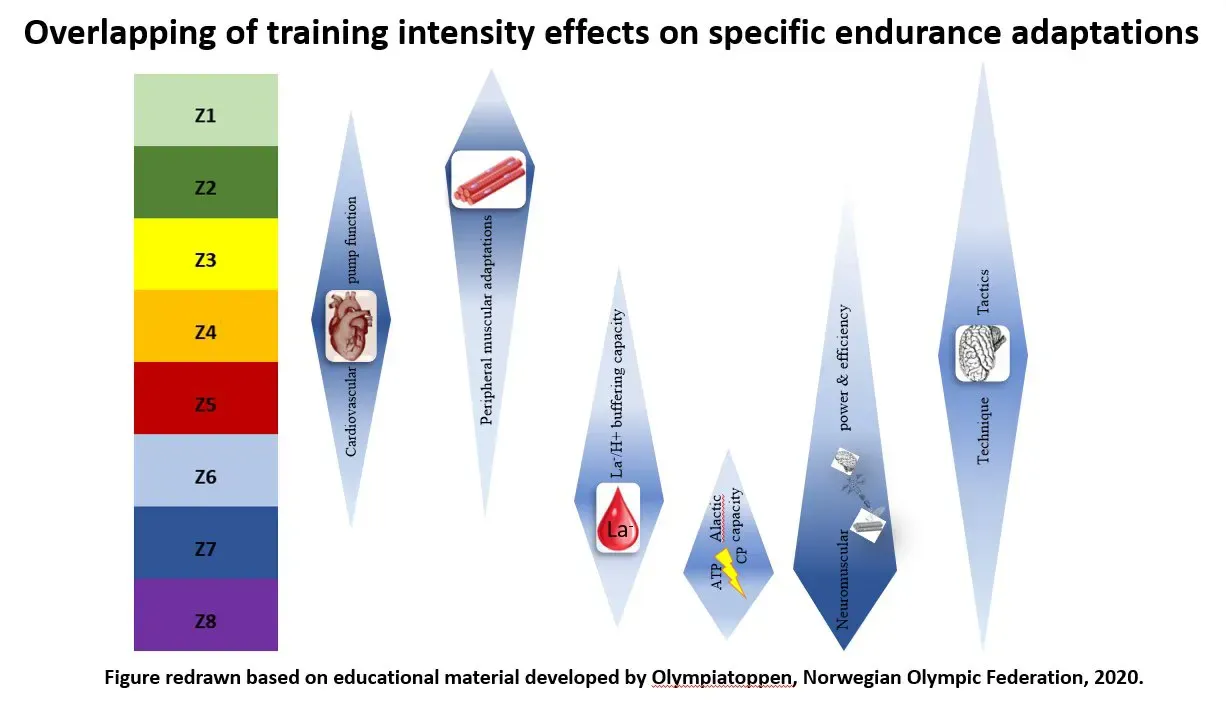
- 進行大量、長時間、舒服不累的低強度有氧,透過時間量的累積,同樣能把心臟幫浦供血功能(心搏輸出量)拉到接近滿分。
- 更重要的是,Zone 2 也是鍛鍊並修復骨骼肌細胞內「粒線體(Mitochondria)」的最佳刺激區間,能大幅優化細胞發電效率與代謝彈性。
- 運動: 超慢跑、慢跑、騎車或游泳。
- Zone 2 訓練強度不高但需要時間(建議每次 40–60 分鐘),過程相對枯燥。經過一兩個月體能適應後,應從超慢跑漸進過渡到真正的慢跑(如 7 分速),避免刺激飽和。
第二階段:VO2 max 間歇訓練
- 訓練強度: 最大心率的 90%–95%。
- 科學原理: 當身體已經做足低中強度訓練打底後,額外加入高強度間歇(HIIT)所帶來的 VO2 max 增幅平均約為 2 mL/kg/min。高強度間歇就像是最後 5% 的「拋光工具」,能幫你打破停滯期、頂高體能天花板,但因為其需要額外的恢復時間,必須有計劃地與 Zone 2 搭配,以避免連續高強度帶來的慢性疲勞與過度消耗。
- 以挪威 4x4 間歇訓練為例: 在充足熱身後,進行4 分鐘高強度(10K 比賽配速) + 3 分鐘低強度動態恢復(慢跑或快走),重複執行 4 組,總時間約 45 分鐘(含前後熱身和伸展)。
- 安全限制: 這對身體與發電系統是極大刺激,每週最多進行 1–2 次即可,也不建議連續兩天進行。
要建構完整的健康儲蓄防禦網,除了透過「低強度打底、高強度拋光」的雙軌策略優化心肺功能外,Peter Attia 也提醒,我們必須規律加入阻力訓練與穩定性訓練。力量訓練能儲蓄肌肉量與骨密度,對抗老年肌少症;而穩定性則是大腦控制身體的基礎,是所有力量與有氧運動的安全地基。
Keep moving and living freely in the marginal decade.
總結
- 建議不要過度執著於VO2 max的精確數字:不論實驗室的CPET或是智慧手錶都有測量的誤差,請用長期趨勢的角度監測 VO2 max,不要被它綁架了!
- 「雙軌複利、兩階段訓練法」:透過規律的 Zone 2 運動,穿插HIIT間歇訓練,就可以穩定安全地提昇自己的VO2 max。
- 雖然 VO2 max 在 30 歲後每十年大約下降 10% ,但大數據與文獻皆證實:無論在哪個年齡層,有規律訓練的人,數據永遠比沒練的人更好!
願我們都能在生命中持續自由
Keep moving and living freely in the marginal decade.
更多運動醫學相關文章
醫學|Move with Flux — 在賀爾蒙之間尋回妳的自由
醫學|Fast or Fed?女性斷食的操作指南
醫學|髂徑束症候群,為什麼「慢跑」反而更痛?
醫學|別讓運動從療癒成為傷害
醫學|淺談增生療法:甜甜的,好得比較快?
參考資料
一、 國際醫學臨床指引、共識與官方權威聲明
- American Heart Association. (2016). Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association. Circulation, 134(24), e653-e699. https://doi.org/10.1161/CIR.0000000000000461
- American Heart Association. (2020). Cardiorespiratory fitness in youth: An important marker of health: A scientific statement from the American Heart Association. Circulation, 142(7), e101-e118. https://doi.org/10.1161/CIR.0000000000000866
- American Heart Association. (2024). Core components of cardiac rehabilitation programs: 2024 update: A scientific statement from the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation, 149(11), e1002-e1022.
- American Society of Nuclear Cardiology. (2023). ASNC Practice Point: Exercise stress testing protocols and clinical implementation. ASNC Guidelines.
- Bozkurt, B., Coats, A., Tsutsui, H., Abdelhamid, M., Adamopoulos, S., Albert, N., Anker, S. D., Atherton, J., Böhm, M., Butler, J., et al. (2021). Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society. Journal of Cardiac Failure, 27(4), 387-413. https://doi.org/10.1016/j.cardfail.2021.01.022
- European Respiratory Society. (2019). ERS technical standard - Reference values for cardiopulmonary exercise testing: Summary report and a call for action. European Respiratory Journal, 53(1), 1801581. https://doi.org/10.1183/13993003.01581-2018
- Fletcher, G. F., Ades, P. A., Kligfield, P., Arena, R., Balady, G. J., Bittner, V. A., Coke, L. A., Fleg, J. L., Forman, D. E., Gerber, T. C., Gulati, M., Madan, K., Rhodes, J., Thompson, P. D., & Williams, M. A. (2013). Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation, 128(8), 873-934. https://doi.org/10.1161/CIR.0b013e31829b5b44
- Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., Lee, I. M., Nieman, D. C., Swain, D. P., & American College of Sports Medicine. (2011). Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Medicine & Science in Sports & Exercise, 43(7), 1334-1359. https://doi.org/10.1249/MSS.0b013e318213fefb
- EuroHeart Writing Committee. (2021). Methodology for the development of international clinical data standards for common cardiovascular conditions: European Unified registry platform. European Heart Journal, 42(32), 3195-3205. https://doi.org/10.1093/eurheartj/ehab341
最大攝氧量預測常模研究
- de Souza e Silva, C. G., Kaminsky, L. A., Arena, R., Christle, J. W., Araujo, C. S., Lima, R. M., Ashley, E. A., & Myers, J. (2018). A reference equation for maximal aerobic power for treadmill and cycle ergometer exercise testing: Analysis from the FRIEND registry. European Journal of Preventive Cardiology, 25(7), 742–750. https://doi.org/10.1177/2047487318763958
- Kaminsky, L. A., Arena, R., & Myers, J. (2015). Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing: Data from the Fitness Registry and the Importance of Exercise National Database. Mayo Clinic Proceedings, 90(11), 1515-1523. https://doi.org/10.1016/j.mayocp.2015.07.027
- Myers, J., Kaminsky, L. A., Lima, R., Christle, J. W., Ashley, E., & Arena, R. (2017). A reference equation for normal standards for VO2 max: Analysis from the Fitness Registry and the Importance of Exercise National Database (FRIEND Registry). Progress in Cardiovascular Diseases, 60(1), 21-29. https://doi.org/10.1016/j.pcad.2017.03.002
- NHANES Registry Group. (2022). Reference equations for peak oxygen uptake for treadmill cardiopulmonary exercise tests based on the NHANES lean body mass equations: A FRIEND registry replication study. PubMed, PMID: 35641299.
心肺運動測試(CPET)量測、驗證與微觀生理機制
- Bongers, B., & Takken, T. (2019). Reference values for cardiopulmonary exercise testing in healthy subjects – an updated systematic review. Expert Review of Cardiovascular Therapy, 17(6), 413–426. https://doi.org/10.1080/14779072.2019.1627874
- Buchfuhrer, M. J., Hansen, J. E., Robinson, T. E., Sue, D. Y., Wasserman, K., & Whipp, B. J. (1983). Optimizing the exercise protocol for cardiopulmonary assessment. Journal of Applied Physiology, 55(5), 1558–1564. https://doi.org/10.1152/jappl.1983.55.5.1558
- Çabuk, R., Alp, E., Murias, J. M., & Karsten, B. (2026). Verification trials can create the illusion of V̇O2max in addition to contributing to its confirmation. Scandinavian Journal of Medicine and Science in Sports, 36(2), e70226. https://doi.org/10.1111/sms.70226
- Costa, V. A. B., Midgley, A. W., Baumgart, J. K., et al. (2021). Is a verification phase useful for confirming maximal oxygen uptake in apparently healthy adults? A systematic review and meta-analysis. PLOS ONE, 16(2), e0247057. https://doi.org/10.1371/journal.pone.0247057
- Costa, V. A. B., Midgley, A. W., Baumgart, J. K., et al. (2024). Confirming the attainment of maximal oxygen uptake within special and clinical groups: A systematic review and meta-analysis of cardiopulmonary exercise test and verification phase protocols. PLOS ONE, 19(3), e0299563. https://doi.org/10.1371/journal.pone.0299563
- Heinonen, I. (2025). Cardiac output limits maximal oxygen consumption, but what limits maximal cardiac output? Experimental Physiology, 110(5), 666-674. https://doi.org/10.1113/EP091594
- Jalanko, P., Haapala, E. A., et al. (2025). Measuring V̇O2max in adolescents: Verification phase and impact of time averaging strategies. European Journal of Applied Physiology, 125(4), 1105-1115. https://doi.org/10.1007/s00421-024-05492-1
- Martin-Rincon, M., & Calbet, J. A. L. (2020). Progress update and challenges on VO2max testing and interpretation. Frontiers in Physiology, 11, 572883. https://doi.org/10.3389/fphys.2020.572883
- Mougin, L., Bailey, S. J., Burnley, M., Pearce, R., Mears, S. A., & Zanini, M. (2025). Factors affecting V̇O2 and fat oxidation responses during step incremental exercise. Scandinavian Journal of Medicine & Science in Sports, 35(11), e16008. https://doi.org/10.1111/sms.70110
- Ozemek, C., Bonikowske, A., Cristle, J., & Gallo, P. (Eds.). (2025). ACSM's guidelines for exercise testing and prescription (12th ed.). Wolters Kluwer.
- Pogliaghi, S., Tam, E., & Capelli, C. (2023). Effect of recovery time on VO2 on-kinetics in humans at the onset of moderate-intensity cycling exercise. European Journal of Applied Physiology, 123(2), 261-270. https://doi.org/10.1007/s00421-022-05057-4
- Seismocardiography prediction algorithm research group. (2025). Accuracy of a clinically applicable method for prediction of VO2max using seismocardiography. FutureMedics, 14(2), 89-97.
- Souren, T., Rose, E., & Groen, H. (2021). Comparison of two metabolic simulators used for gas exchange verification in cardiopulmonary exercise test carts. Frontiers in Physiology, 12, 667386. https://doi.org/10.3389/fphys.2021.667386
- Wikipedia contributors. (2026, March 3). Cardiopulmonary exercise test. In Wikipedia, The Free Encyclopedia. Retrieved June 22, 2026, from https://en.wikipedia.org/wiki/Cardiopulmonary_exercise_test
- Wikipedia contributors. (2026, January 18). Bruce protocol. In Wikipedia, The Free Encyclopedia. Retrieved June 22, 2026, from https://en.wikipedia.org/wiki/Bruce_protocol
運動訓練組織、高強度間歇與表現適應(HIIT vs. SIT)
- Bacon, A. P., Carter, R. E., Ogle, E. A., & Joyner, M. J. (2013). VO2max trainability and high intensity interval training in humans: A meta-analysis. PLOS ONE, 8(9), e73182. https://doi.org/10.1371/journal.pone.0073182
- Gentil, P., et al. (2019). Effect of high-intensity interval training versus sprint interval training on time-trial performance: A systematic review and meta-analysis. Journal of Strength and Conditioning Research, 33(12), 3452-3461.
- Granata, C., Jamnick, N. A., & Bishop, D. J. (2018). Principles of exercise prescription and how they influence exercise-induced changes of transcription factors and other regulators of mitochondrial biogenesis. Sports Medicine, 48(7), 1541–1559. https://doi.org/10.1007/s40279-018-0915-9
- Mujika, I. (Ed.). (2024). Endurance Training: Science and Practice (2nd ed.). Inigo Mujika Publishing. (訓練效果「區間重疊性」Figure 4.3 核心文獻).
- Tucker, W. J., Fegers-Wustrow, I., Halle, M., Haykowsky, M. J., Chung, E. H., & Kovacic, J. C. (2022). Exercise for primary and secondary prevention of cardiovascular disease: JACC Focus Seminar 1/4. Journal of the American College of Cardiology, 80(11), 1091-1106. https://doi.org/10.1016/j.jacc.2022.07.004
- Vilaça-Alves, J., Silva, C. A., Monteiro, E. R., Vianna, J., Novaes, J., Garrido, N., & Reis, V. (2026). Comparing the effects of simultaneous execution versus isolated training on oxygen consumption during exercise. Retos, 80, 185-192. https://doi.org/10.47197/retos.v80.118687
- Zhang, X., Weakley, J., Li, H., Li, Z., & García-Ramos, A. (2025). Superset versus traditional resistance training prescriptions: A systematic review and meta-analysis exploring acute and chronic effects on mechanical, metabolic, and cardiovascular responses. Journal of Strength and Conditioning Research, 39(1), 112-124.
長壽醫學、抗老機制、肌少症與大眾科學傳播
- Alkan, M., et al. (2024). Digitisation and linkage of PDF formatted 12-lead ECGs in Adult Congenital Heart Disease. arXiv preprint, arXiv:2503.14239v1 (published online March 18, 2025).
- Attia, P. (2023). Outlive: The Science and Art of Longevity. Harmony Books.
- Attia, P. (2024). An Introductory Guide to Longevity: Medicine 3.0 and the Centenarian Decathlon. Early Medical E-books.
- Dungan, C. M. (2025). Myonuclear dynamics with age and exercise: Shaping up for a good time. The Journal of Physiology, 603(13), 3859-3860. https://doi.org/10.1113/JP284303
- The Economist. (2026, February). Kristian Blummenfelt, the Norwegian athletic miracle, and the rise of VO2 max tracking algorithms. The Economist Special Report.